BLOG
Same-Day Tooth Extraction and Immediate Implant Placement: Workflow and Training Insights
Blog Tarihi: 14/06/2026

Same-day extraction and immediate implant placement: what it means
“Same-day tooth extraction and implant” commonly refers to extracting a hopeless tooth and placing a dental implant into the fresh socket during the same appointment—often called immediate implant placement. In selected patients, this approach can reduce total treatment time, preserve soft-tissue contours, and streamline the path to a functional and aesthetic restoration. However, it is not a universal solution; predictability depends on diagnosis, tissue conditions, surgical skill, and prosthetic planning.
For a patient-friendly overview of the concept of accelerated implant timelines, see Is One-Day Dental Implant Treatment Really Possible?. For clinicians seeking a structured, step-by-step overview of immediate placement principles, you can also reference Same-Day Tooth Extraction and Immediate Implant Placement: A Clinical Guide.
This content is for educational purposes only. Clinical decisions should be made by qualified dental professionals based on individual patient evaluation, imaging, systemic factors, and current evidence.
Why consider immediate implant placement?
Potential clinical and patient-centered advantages
When performed under appropriate conditions, immediate placement may offer:
• Fewer surgical appointments: extraction and implant placement are combined into one surgical visit.
• Preservation of anatomy: socket-guided placement may help maintain ridge contour, especially in the aesthetic zone, when combined with appropriate grafting/contouring strategies.
• Earlier prosthetic planning: restorative considerations can guide implant positioning from day one, aligning with a prosthetically driven workflow.
• Improved patient acceptance: some patients prefer consolidated timelines and fewer procedures.
What “same-day” is (and is not)
In education and marketing, “same-day” can be misunderstood. Same-day extraction + implant placement does not automatically mean same-day final crown. A provisional restoration may be possible in select cases (often termed immediate provisionalization), but only when stability and occlusal risk are appropriately managed. The definitive restoration typically follows healing and integration protocols, and the timeline varies.
Case selection: the cornerstone of predictability
The most sophisticated surgical technique cannot compensate for a poorly selected case. Immediate implants are generally considered when infection control, socket morphology, bone volume, and patient risk profile support primary stability and soft-tissue management.
Clinical indications often considered
Immediate placement may be considered (depending on clinician judgment and evidence-based protocols) when:
• The tooth is non-restorable due to fracture, extensive caries, or failed endodontic/restorative prognosis.
• Adequate apical/palatal bone exists to achieve primary stability beyond the socket.
• Soft tissues are manageable with an acceptable gingival phenotype and controllable recession risk.
• The patient’s systemic and behavioral factors support healing (e.g., controlled medical conditions, realistic expectations, acceptable oral hygiene).
Key contraindications and risk amplifiers
While not an exhaustive list, clinicians often exercise caution with:
• Uncontrolled periodontal disease or poor plaque control.
• Severe acute infection with compromised socket walls (case-dependent).
• Inadequate bone for stability (thin buccal plate, large defects, insufficient apical anchorage).
• High esthetic risk (thin biotype, existing recession, high smile line) without a robust soft-tissue plan.
• Occlusal/parafunctional risk if immediate provisionalization is planned.
Because soft-tissue stability is frequently the limiting factor in the anterior region, understanding recession patterns and periodontal risk assessment is crucial. A deeper discussion is available in Gum Recession: Causes, Symptoms, and Evidence-Based Management.
Preoperative planning: diagnosis, digital tools, and interdisciplinary thinking
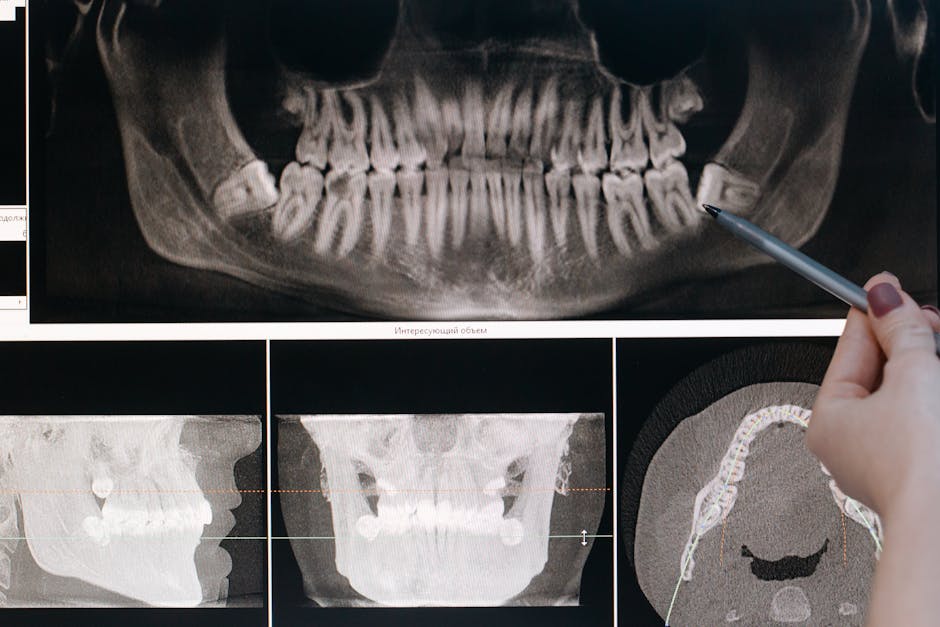
Imaging and diagnostics
A thorough diagnostic phase typically includes a clinical exam, periodontal charting, occlusal analysis, and radiographic assessment. In many immediate implant workflows, CBCT supports three-dimensional evaluation of socket walls, buccal plate thickness, anatomic limitations, and the available apical bone needed for stability. Intraoral scans and digital wax-ups can further align implant placement with restorative goals.
Prosthetically driven positioning
Immediate placement is most predictable when the implant is placed where the restoration needs it—not simply where bone is easiest. This is the logic behind prosthetically driven implant dentistry: emergence profile, contact points, and crown contours are planned first, and the implant is positioned accordingly. Digital planning and guided surgery may support this approach, particularly for clinicians building consistency in anterior cases.
Aesthetic context: smile design and patient expectations
In the aesthetic zone, the implant is part of a broader smile framework: midline, incisal plane, gingival architecture, and tooth proportions all matter. Some patients exploring immediate implants are also interested in comprehensive aesthetic treatment plans (e.g., veneers, whitening, or full smile rehabilitation). For an evidence-informed overview of aesthetic workflows and materials, see What Is a Hollywood Smile? Techniques, Materials, and Clinical Workflow.
Clinical workflow: from atraumatic extraction to implant placement
Protocols vary by clinician preference and patient needs, but immediate implant placement often follows a consistent sequence.

1) Atraumatic extraction and socket preservation mindset
The goal is to remove the tooth while preserving the socket walls—especially the buccal plate. Periotomes, sectioning techniques, and controlled force help reduce trauma. In educational settings, dentists often practice extraction techniques on models/cadavers to improve tactile control and minimize complications.
2) Debridement and assessment of socket integrity
After extraction, the socket is carefully debrided to remove granulation tissue and evaluate the condition of the walls. This step also provides real-time information that may change the plan (e.g., converting an immediate approach to an early/delayed protocol if stability or defects are unfavorable).
3) Osteotomy and 3D implant positioning
Primary stability is typically obtained by engaging bone beyond the apex or along palatal/lingual aspects, depending on the tooth and arch. Clinicians aim to manage:
• Depth: supporting an appropriate emergence profile and avoiding a “too shallow” placement that risks aesthetic compromise.
• Buccal-lingual position: avoiding excessive buccal placement that can increase recession and bone loss risk.
• Angulation: aligning restorative access and load distribution.
4) Gap management and grafting concepts
Because the socket often has a horizontal gap between implant and socket wall, clinicians may consider grafting strategies to support contour and soft-tissue stability. The choice of biomaterial and technique is case-dependent and should be guided by current evidence and training.
5) Soft-tissue management and phenotype considerations
Soft-tissue thickness and keratinized tissue can influence long-term aesthetics and peri-implant health. In certain situations, clinicians may consider soft-tissue augmentation techniques to improve tissue volume and resilience. Educational resources discussing biomaterials used in soft-tissue procedures can be found in Asellüler Dermal Matriks: Diş Hekimliğinde Kullanımı, which explores how acellular dermal matrices are applied in dentistry (within the boundaries of clinician judgment and appropriate indications).
6) Provisionalization: when (and why) it may be considered
Immediate provisional restorations can help shape soft tissue and support patient comfort and aesthetics—particularly in anterior cases. Yet, provisionalization should be approached cautiously and typically requires excellent primary stability and carefully controlled occlusion to limit micromovement. In many cases, clinicians choose a healing abutment or a customized provisional that avoids occlusal contact.
Postoperative considerations: healing, monitoring, and long-term maintenance
After surgery, structured follow-up is essential. Clinicians monitor soft-tissue maturation, plaque control, occlusion, and signs of inflammation. Final restoration timing is individualized. Peri-implant health is influenced by patient-level factors (home care, smoking, systemic conditions), prosthetic contours, and maintenance protocols.

From an educational standpoint, this phase is where restorative dentistry, periodontology, and prosthodontics converge: emergence profiles, cleansability, and material selection can either protect tissues or create chronic inflammation risk.
Common pitfalls in same-day extraction and immediate implants (and how training helps)
Esthetic complications from poor 3D placement
Even with integration, implants placed too buccally or shallow may compromise gingival margins and emergence profile. Digital planning, surgical guides, and restorative mock-ups can reduce these errors—when used with appropriate training.
Overpromising timelines
Patients may interpret “same-day” as immediate final results. Ethical communication matters: dentists should explain that immediate placement does not guarantee immediate loading, and that biology and risk management dictate the pace.
Underestimating periodontal and recession risks
Thin biotype, existing recession, or active periodontal problems can undermine the aesthetic outcome. A thorough periodontal assessment and soft-tissue strategy should be part of the plan, not an afterthought.
How Istanbul Dental Academy supports clinical competence in immediate implant workflows
Immediate implant placement is a technique-sensitive procedure that benefits from structured education: diagnosis, CBCT interpretation, flap design options, suturing, soft-tissue management, and prosthetically driven planning. At Istanbul Dental Academy, our continuing dental education approach emphasizes hands-on skill development—helping dentists translate theory into predictable clinical workflows in implant dentistry, oral surgery, periodontology, restorative dentistry, and prosthodontics.
Courses commonly integrate digital dentistry components (intraoral scanning, smile planning, guided surgery concepts) alongside surgical fundamentals such as atraumatic extraction and socket management. For many clinicians, pairing these skill sets is what enables confident decision-making—knowing when immediate placement is appropriate and when alternative timing is safer.
Key takeaways
• Same-day extraction and implant placement can be feasible in selected cases with robust diagnosis and planning.
• Soft tissue and 3D placement drive aesthetics, especially in the anterior region.
• Digital tools support consistency, but they do not replace surgical fundamentals.
• Training and mentorship matter—particularly for managing complications, tissue phenotype, and prosthetic-driven positioning.
If you are a dentist or dental student aiming to build competence in immediate implant placement—understanding not only the “how,” but also the “when” and “why”—a structured, hands-on learning pathway can shorten your clinical learning curve while improving patient communication and outcomes. This article is for educational purposes and is not a substitute for individualized clinical training or patient-specific treatment planning.
Diğer Yazılar






















































